TRAM FLAP FOR BREAST MOUND RECONSTRUCTION
The Transverse Rectus Abdominus Myocutaneous flap sacrifices one or both rectus abdominus muscles (the sit-up muscles) to supply the blood flow to the overlying skin and fat that will be used to form the breast.
These muscles have a dual blood supply: there are vessels that enter the upper muscle just below the rib cage, and there are vessels that enter the muscle from the groin. The flap that is utilized to make the breast is the skin and fat between the belly button and the pubic area. The blood supply to the lower abdominal skin and fat is dominantly supplied by the lower, and not the upper set of blood vessels. The upper blood vessels are used for the pedicled TRAM flap; the lower are used for the free TRAM flap.
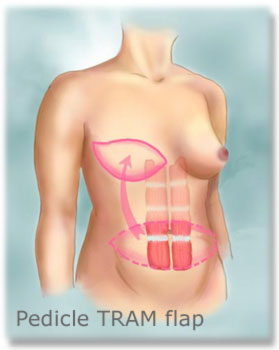
With the pedicled TRAM flap, the skin and fat are left attached to the lower portion of one rectus muscle. The muscle inferior to the skin and fat that will be used to form the new breast is cut, leaving the blood supply at the level of the rib cage intact. The skin, fat, and muscle are then lifted up and tunneled beneath the upper abdominal skin to the chest. There, the skin and fat are shaped into a breast. The scar that results from the TRAM flap is identical to the one seen after abdominoplasty (a tummy tuck). The scar lies transversely (from side to side) across the lower abdomen, typically situated just above the pubic hair line (as shown in our second drawing). During creation of the flap the belly button is left attached to the abdominal wall. When the skin of the upper abdomen is stretched to close the resulting abdominal wound the belly button is repositioned to an anatomic location.
The free TRAM flap is a significant improvement over the traditional procedure. in this procedure, the skin and fat of the lower abdomen used to form the breast are left attached to one rectus muscle. The portion of muscle above and below the attached skin and fat is divided. The flap is removed with its blood vessels, positioned on the chest and then with microsurgery the blood vessels are reattached to provide blood flow to the transferred flap. It is called a free flap because the piece of tissue is truly free just before transfer. Besides the advantage of using a more dominant blood supply (and therefore having a more reliable flap) since there is no tunneling there is not a bulge in the upper abdomen.
Because of the magnitude of the procedure, complications can occur even in the best of hands. Possible complications from a TRAM flap procedure are listed below.
- Fat necrosis and/or partial flap loss (5-15% of patients)
- Complete loss of TRAM tissue (<1% of patients)
- Seroma (fluid collection, usually in abdominal donor site)
- Hematoma (bleeding at either chest or abdomen)
- Infection
- Hernia (1-5% of patients)
- Abdominal bulge without hernia (5-15% of patients)
- Deep venous thrombosis and/or pulmonary embolus (<1% of patients)
- Death (<1% of patients)
Since the TRAM flap has its own blood supply, and transfers new tissue to create the reconstructed breast, it is also very useful in the situation of breast reconstruction after radiation. Women who have had radiation for treatment of their breast cancer are not candidates for tissue expansion/breast implants, and therefore need a flap reconstruction of some kind.
| Latissimus Flaps: | TRAM Flaps: |
|---|---|
| What is the latissimus flap?The latissimus is the large muscle on the upper back. This flap uses that muscle and a portion of the overlying skin and fatty tissue to recreate the breast mound. | What is the TRAM flap?This flap takes one or both of the rectus abdominis muscles along with a large section of overlying skin and fatty tissue from the lower abdomen to recreate the breast mound. |
Pros:
|
Pros:
|
Cons:
|
Cons:
|